About ANCA-Associated Vasculitis (AAV)
Common Symptoms
- Constitutional symptoms
- Eye redness and pain
- Nasal/sinus symptoms (nasal congestion, bleeding, drainage, pressure)
- Pulmonary (cough, shortness of breath)
- Renal (glomerulonephritis)
Granulomatosis with Polyangiitis (GPA)
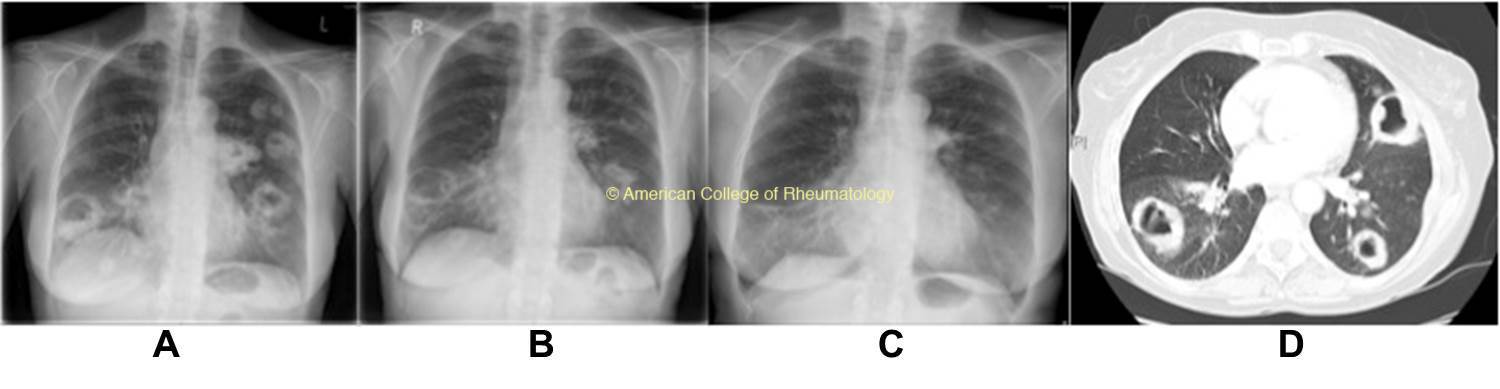
- Cavitary pulm lesions
- Upper airway limited (ANCA neg)
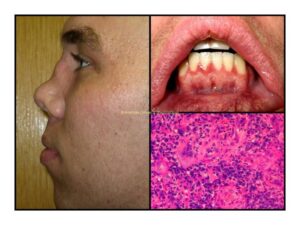
- Sinonasal disease with chronic sinusitis, epistaxis, saddle nose deformity (view image)
- Pseudotumor
- Nasal septal or palate perforation (view image)
- Tracheal/subglottic stenosis
Microscopic Polyangiitis (MPA)
- Pulm-renal
- (ANCA pos when renal disease)
- Pulm-renal on histopathology doesn’t have granulomas
Eosinophilic Granulomatosis with Polyangiitis (EGPA)
- Allergic rhinitis (often with nasal polyps)
- Asthma (often adult-onset)
- Peripheral and tissue eosinophilia
- Vasculitis that can frequently involve the skin and nerves
- Cardiac involved (ANCA neg) – can be life-threatening:
- Pericardial effusion
- Myocarditis
Lab Workup
- CBC with differential, chemistries, ESR/CRP (high), creatinine, urinalysis
- ANCA panel (most common association)
- Anemia of chronic disease
- AKI
- Urinalysis:
- +blood
- +protein
- +RBC casts
Imaging
- CXR/CT chest (view images)
- Diffuse infiltrates in diffuse alveolar hemorrhage (DAH)
- Cavitating lung lesions in GPA
Bronchoscopy
- Confirm DAH
- Rule out infection (bacterial, fungal)
- Rule out malignancy
Kidney Biopsy
- Pauci-immune crescentic glomerulonephritis (GN)
Drug Induced
- PTU
- Hydralazine
- Minocycline
- Levamisole
Malignancy
Infection
-
Infective endocarditis
-
Organisms that can cause cavitary lung lesions and lung abscesses (tuberculosis, aspergillosis, pseudomonas, etc.)
Other Kidney Disease
- Lupus nephritis
- Membranous nephropathy
- IgA nephropathy
- Post-infectious glomerulonephritis (GN)
- Goodpasture (GBM disease)
Other Rheumatic Diseases
-
Cryoglobulinemic vasculitis
-
Antiphospholipid syndrome
-
Complement-mediated disease
Other Vasculopathies
-
Cocaine-associated vasculopathy
-
Microthrombi leading to vasculopathy
- Should be managed in conjunction with a rheumatologist, nephrologist, or other specialist experienced with these diseases
- Two-part approach: induction and maintenance
Induction
- High doses of steroids (500-1000 mg IV for 3-5 days) followed by taper
- Consider treatment for glucocorticoid-induced osteoporosis
- Cyclophosphamide
- IV intermittent dosing or PO daily
- Mesna to mitigate risk of hemorrhagic cystitis
- Due to risk of infertility, prior to administration:
- Women of child-bearing age: consider ovarian preservation
- Men: sperm banking
- Rituximab
- IV
- Noninferior efficacy to cyclophosphamide but safer
- Methotrexate (for localized, milder disease – i.e., upper respiratory-limited GPA)
- PO weekly or SQ
- +/- plasma exchange
- Reserved for specific clinical scenarios
- Avacopan as add-on therapy for those with severe active disease
Maintenance Choices
- Azathioprine
- Methotrexate (works well for sinonasal/upper airway disease)
- Rituximab
- IV
- Associated with lower risk of relapse compared to azathioprine
Additional Therapy
Monitoring
- For patients with lung disease and/or receiving remission induction treatment (e.g., rituximab, cyclophosphamide)
- Pneumocystis jiroveci pneumonia (PJP) prophylaxis needed
- Monitor CBC every 1-2 wks with cyclophosphamide use
- Monitor renal function with metabolic panel and creatinine, urinalysis for proteinuria+hematuria
- Monitor pulmonary function with respiratory symptoms, physical exam and PFTs +/- imaging, as needed
- Monitor for infection from systemic immunosuppressive medications
Prognosis
- 80-90% mortality risk if untreated
-
Need for dialysis in setting of renal disease can contribute significantly to mortality and morbidity
Disease Overview & Clinical Presentation
- Adult with new-onset asthma: consider eosinophilic granulomatosis with polyangiitis (EGPA)
- Keep granulomatosis with polyangiitis on DDx for:
- New diagnosis of otitis media as adult
- Recurrent sinusitis +/- epistaxis
- Pseudotumor
- Nasal septal perforation (view image)
- Pulmonary renal syndrome
- Vasculities often presents with:
- C-ANCA or PR3-ANCA = GPA (less commonly EGPA or MPA)
P-ANCA or MPO-ANCA = MPA - Look for potential medications for drug-induced vasculitis
- ANCA negative does not rule out AAV
- ANCA usually negative in cardiac-associated EGPA or upper airway limited GPA