About Rheumatoid Arthritis
Rheumatoid arthritis (RA) is an inflammatory, autoimmune disease primarily impacting the joints.
- F:M = 3:1
- Onset: 20-30 yo and a second spike in early 60s
- Interplay of environment and genetics:
- Smoking
- Oral bacteria
- Shared epitope: HLA-DR1 or DR4
- Onset insidious, usually >=6 weeks
- Symmetric, polyarthritis
- Usually small joints
- >1 hour morning stiffness
- Stiffness improves with activity
- Involving: wrists, MCPs, PIPs, MTPs (5th MTP), knees, ankles, C1/C2 subluxation
- Associated with fatigue and sometimes low grade fever
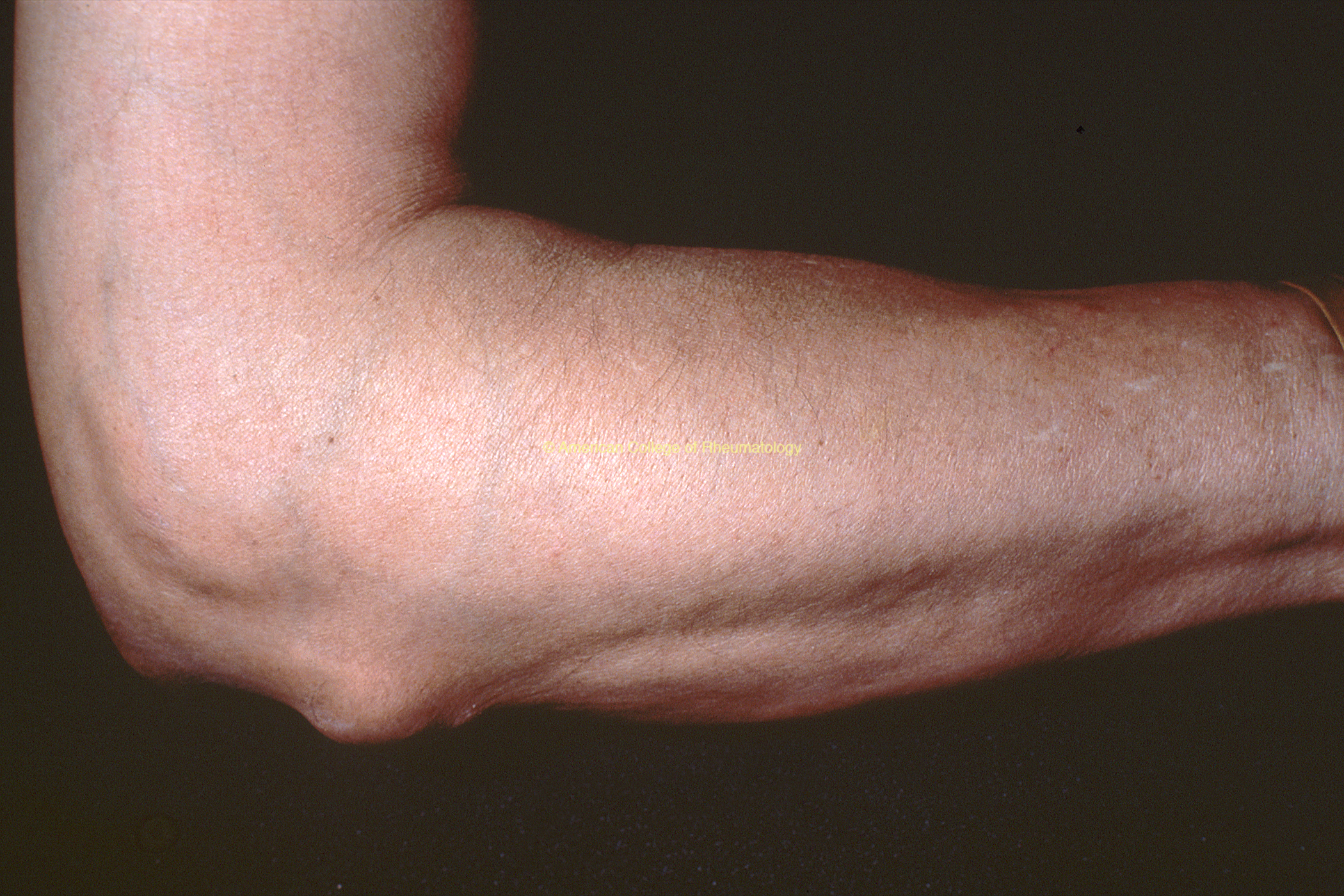
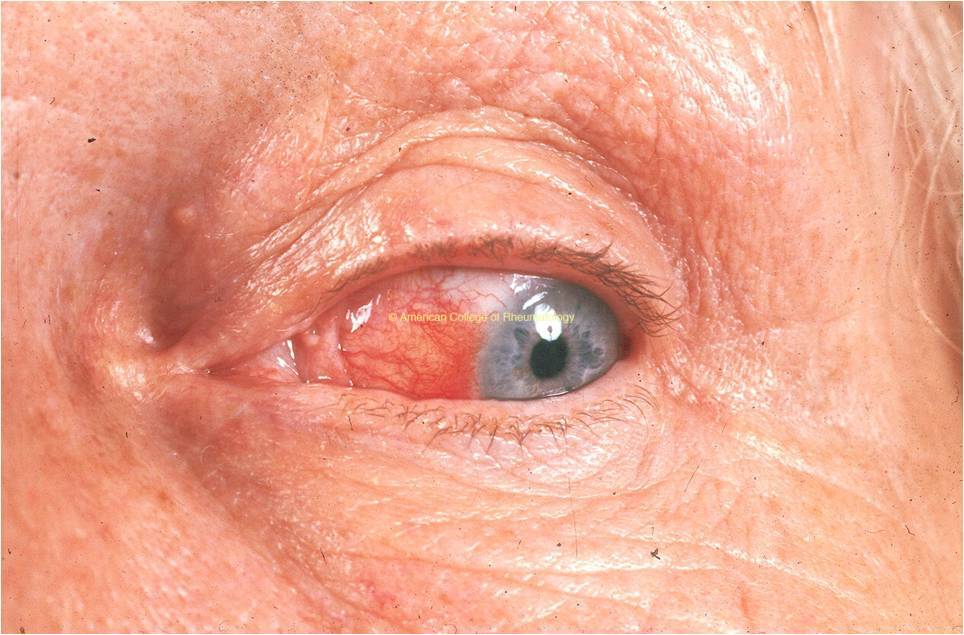
- Extra-articular
- RA nodule (view images)
- Sicca
- Raynaud’s
- Pleural effusion (low glucose)
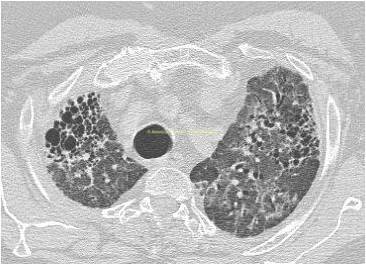
- Fibrotic ILD
- Scleritis (view image)
Lab Workup
- Rheumatoid factor (RF): moderate sensitivity (negative in about 20% of patients) and limited specificity (can be positive in hepatitis, bacterial endocarditis, etc.)
- Citrullinated cyclic peptide (CCP): very specific, predictive
- C-reactive protein and ESR both very sensitive for inflammation but non-specific for RA
- Anemia of chronic disease
Synovial Fluid
- 2k-50k/mL neutrophilic
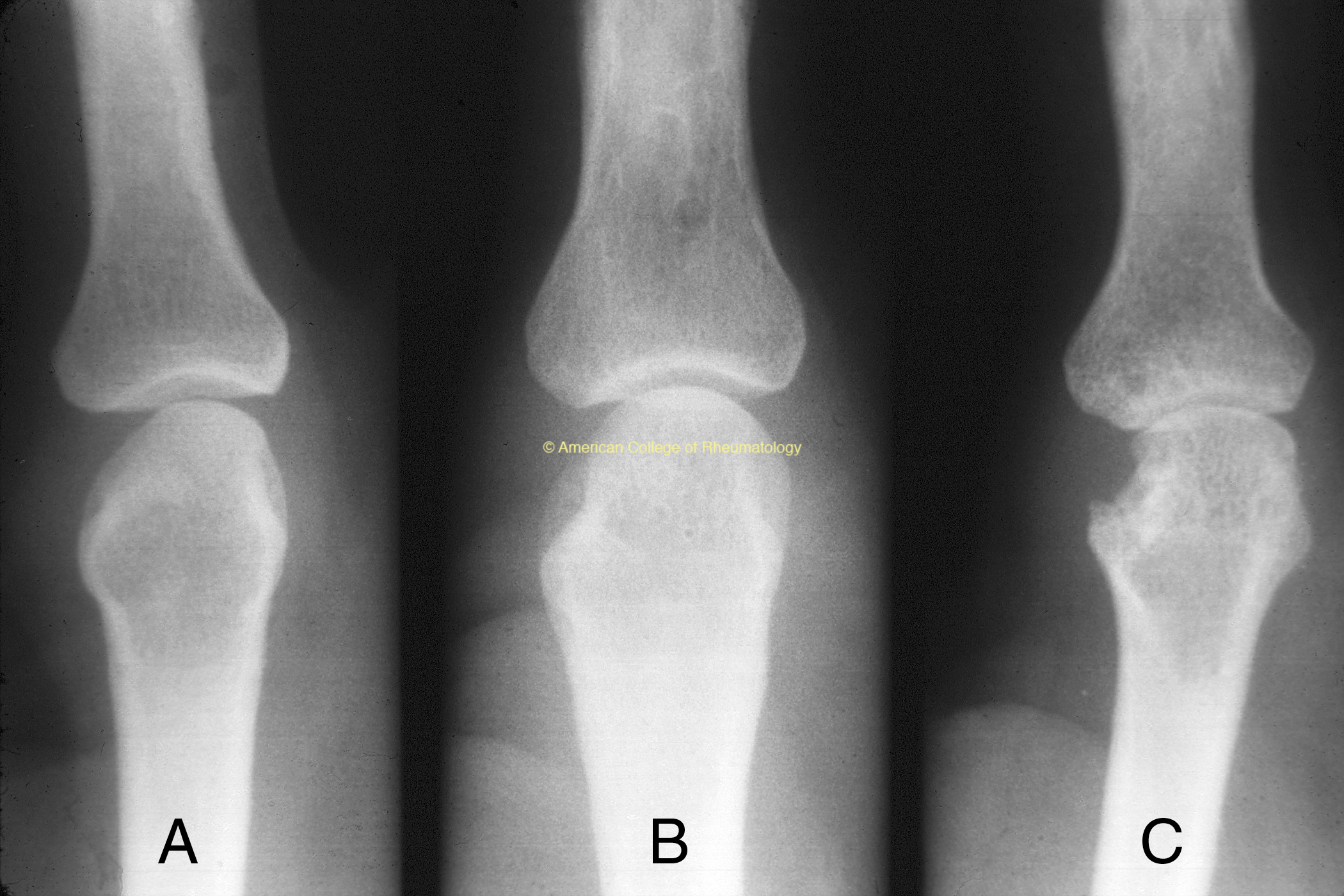
Imaging
- Hand and feet x-rays (view image)
- 3-views: marginal erosions (view image), late RA-subluxation
Other Rheumatic Disease
- Lupus
- Seronegative spondyloarthritis
- Especially psoriatic arthritis
- Crystal arthritis:
- Gout
- Pseudogout
Viral Arthritis
- Parvovirus B19
- Hepatitis B, C
Sarcoidosis
Endocrinopathy
- Thyroid disease
- Hemochromatosis (MCP 2/3)
Short-Term Therapy
Quick onset, unsafe in high doses long term
- NSAIDs: symptom relief only; NSAIDS do not slow/modify disease
- Celebrex, diclofenac, naproxen
- Usually oral; dosing depends on agent
- Glucocorticoids: have some potential to slow/modify disease (weak DMARDs)
- Hydrocortisone, PO or IV
- Methylprednisolone, PO, SQ or IV
- Prednisone, PO only
Long-Term Therapy
DMARD = disease-modifying anti-rheumatic drugs (DMARDs)
Conventional Disease Modifying Anti-Rheumatic Drugs (cDMARDs)
- Hydroxychloroquine: QD or BID PO
- Generally well tolerated
- To reduce risk of retinal toxicity, limit to ≤5 mg/kg daily
- QTc prolongation may occur
- Leflunomide: QD PO
- Teratogenic
- Methotrexate: Weekly PO or SQ with folic acid
- Teratogenic
- CMP monitoring
- Sulfasalazine: BID PO
- Check G6PD prior
- Azathioprine: BID PO
- Check TPMT prior
Biologic Disease Modifying Anti-Rheumatic Drugs (bDMARDs)
Large molecules so have to be injections: subcutaneous (SQ) or intravenous (IV) administration
- TNF-alpha inhibitors
- Adalimumab, SQ
- Certolizumab pegol, SQ
- Etanercept, SQ
- Golimumab, SQ or IV
- Infliximab, IV
- B-cell targeting medications
- Rituximab, IV
- IL6 axis inhibitors
- Sarilumab, SQ
- Tocilizumab, SQ or IV
- CTLA4 agonist
- Abatacept, SQ or IV
Targeted Synthetic Disease Modifying Anti-Rheumatic Drugs (tsDMARDs)
Small molecule so oral, but unlike the conventional DMARDs as they are targeted to a particular molecule
- JAK inhibitors
- Baricitinib
- Tofacitinib
- Upacitinib
Occupational therapy/physical therapy are vital.
- Goal of early inflammation suppression
- Prevent joint damage (damage is irreversible)
- Lower CV risk
- Complications
- Inflammatory lung disease (view image)
- Vasculitis
- AA amyloid
Disease Overview & Clinical Presentation
- Low grade fever can occur
- 5th MTP most common joint affected with RA (view image)
- C1/C2 subluxation is a complication
- Spares DIPs, thoracic and lumbar spine
Diagnostic Workup & Differential Diagnosis
- Rheumatoid factor (RF) sensitive: If low-positive and low suspicion of RA, check hepatitis serologies
- Citrullinated cyclic peptide (CCP): Specific and predictive
- Early x-rays: Marginal erosions, osteopenia
Late x-rays: Subluxuation, osteoporosis
Treatment
- Glucocorticoids: Weak DMARDs if NSAIDs didn’t modify disease -> NSAIDs are not DMARDs
- Glucocorticoids are effective symptom relievers and weak DMARDs, and may serve as a good bridging agent if NSAIDs are not adequate until more potent DMARDs can take effect. However, glucocorticoids have many long-term adverse effects, and the goal should be to use them at as low a dose and for as short a time as possible.
- Methotrexate is gold standard, first line