About Polyarteritis Nodosa
Polyarteritis nodosa (PAN) is a necrotizing systemic vasculitis affecting the medium sized vessels.
- Rare (incidence 1-10/million)
- M:F ratio = 1.5:1
- Onset usually in middle age (40-60 yo)
- Largely idiopathic, but there is an association with HBV infection
General Presentation
- Usually subacute onset
Very Common
- Constitutional: weight loss +/- fevers and night sweats
- ESR/CRP elevation
- Anemia, leukocytosis
Specific Organ Involvement Varies
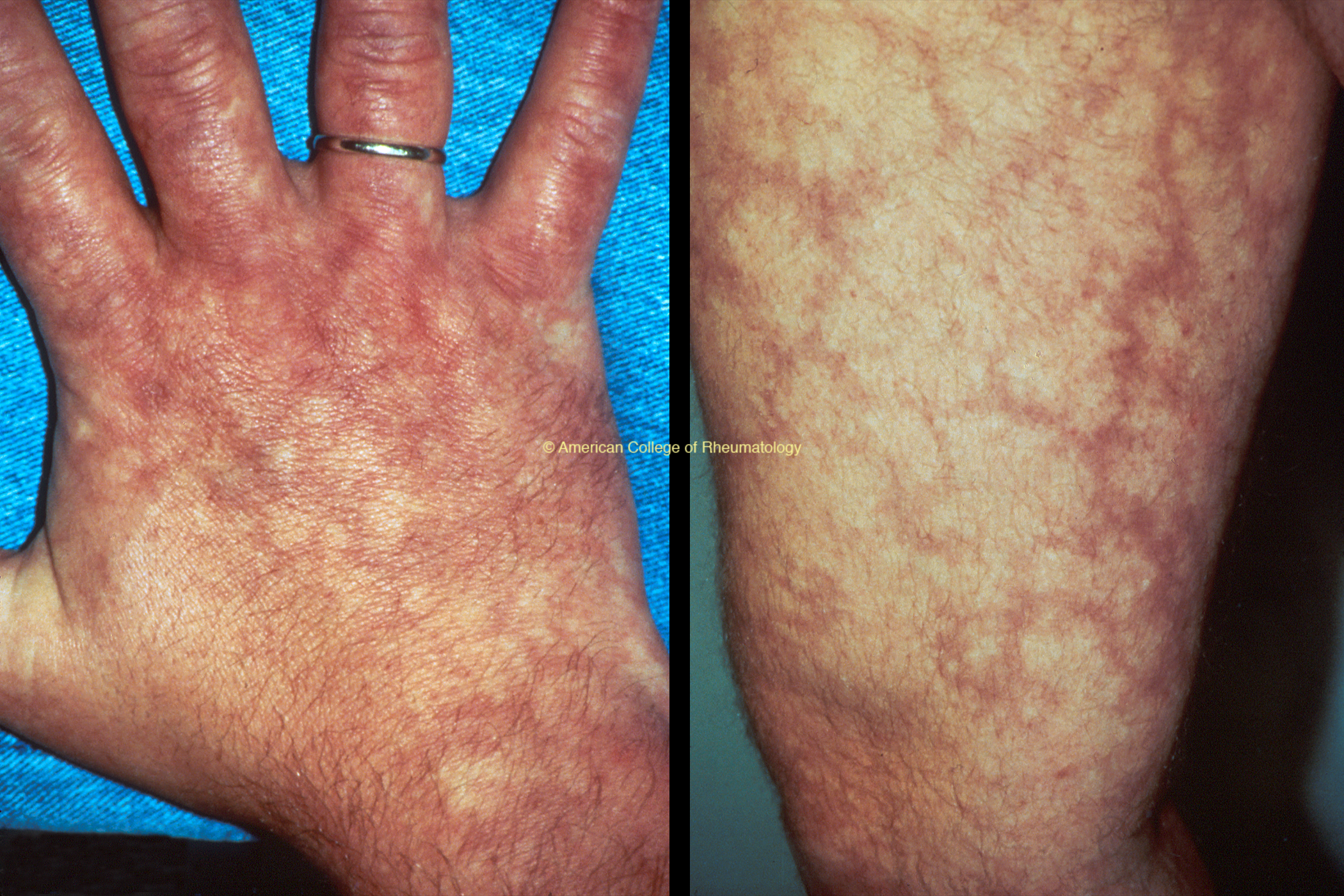
- Skin (livedo, ulcers, nodules, digital ischemia) (view image)
- Neuropathy (especially mononeuritis multiplex) (view image)
- Symptoms of medium vessel vasculitis, renal/mesenteric arteritis: abdominal pain, unexplained hypertension
- Myalgia (especially lower extremities)
- Severe testicular pain and/or enlargement
- Tends to spare the lungs (does not cause diffuse alveolar hemorrhage)
- Does not cause glomerulonephritis
Labs
- CBC w/ diff, CMP, ESR, CRP
- Hepatitis serologies to check for active infection
- Urinalysis to look for RBC casts or proteinuria
- If RBC casts, diagnosis is not PAN
Imaging
- Imaging of medium-sized arteries with CT angiogram, MRA, or conventional angiography will show vasculitis with microaneurysms (view image)
Biopsy
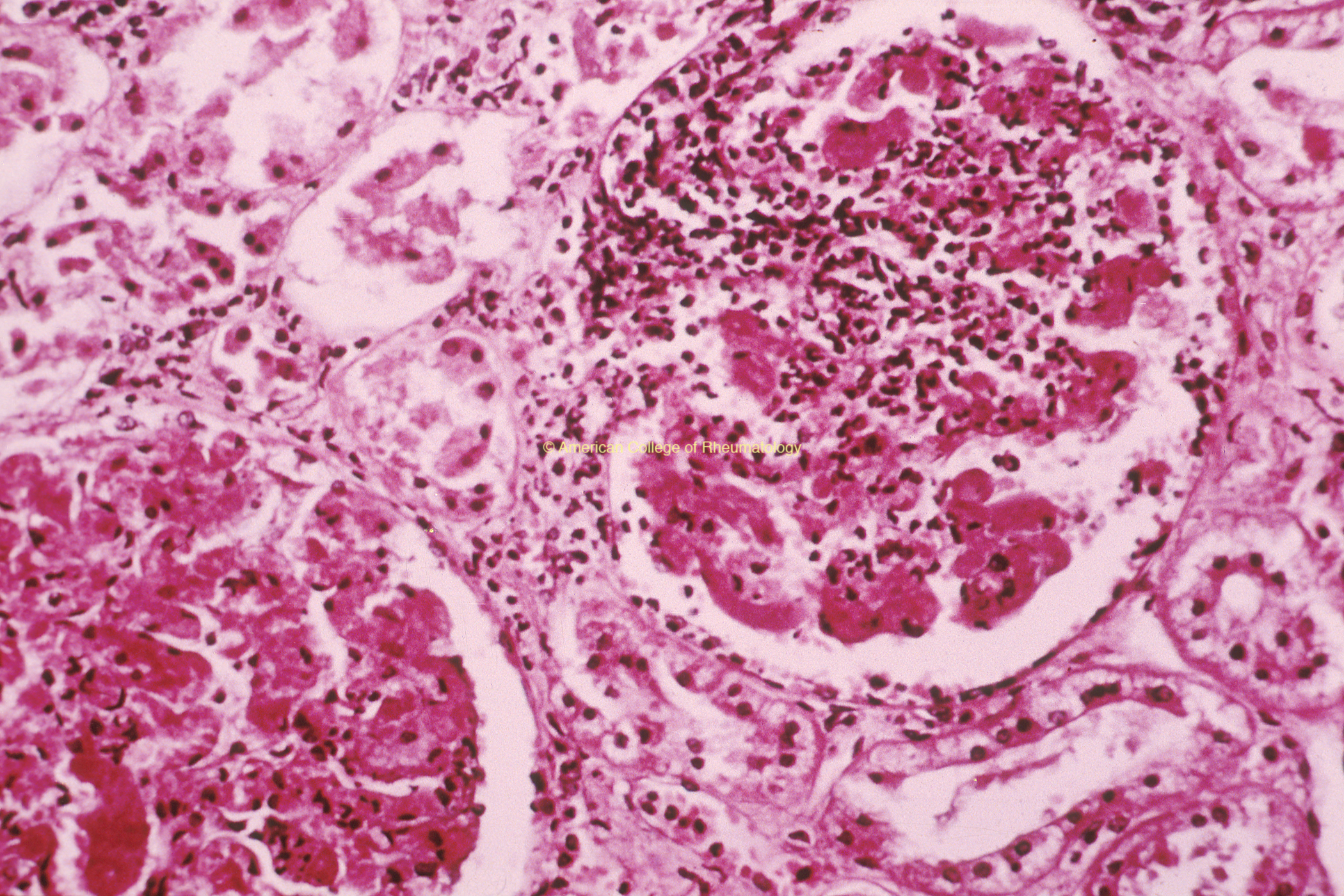
- Cutaneous ulcer or nerve biopsy showing necrotizing medium vessel vasculitis
Other Vasculitides
- ANCA-associated
- Giant cell arteritis (GCA)
- Thromboangiitis obliterans
- Cryoglobulinemic vasculitis
- Antiphospholipid syndrome
Infections
- Endocarditis
- Mycotic aneurysm
Malignancy
- Leukemia
- Lymphoma
- Atrial myxoma
Vasculopathies
- DADA
- Fibromuscular dysplasia
- Segmental arterial mediolysis,
- Collagen-vascular disorders (Vascular Ehlers Danlos syndrome, etc.)
Treatment by rheumatologist needed
- Moderate-high dose steroids plus another “steroid-sparing” immunosuppressive
- Common steroid-sparing agent for PAN: cyclophosphamide
- Identify if associated hepatitis B and treat HBV
- If so, collaboration with ID important
- Disease may be monophasic.
- Drug-free remission is possible.
Disease Overview & Clinical Presentation
- DDx: Infection or malignancy
- PAN spares the lung or renal parenchyma:
- PAN doesn’t present with diffuse alveolar hemorrhage
- PAN doesn’t present with glomerulonephritis (GN)
Diagnostic Workup
- CRP, ESR high, but otherwise labs limited value
- Biopsy is vital if possible
- Imaging: CTA, MRA
- Consider invasive angiography if bx not possible
Treatment and Monitoring
- Aggressive immunosuppression needed for treatment
- Monitor for treatment toxicity (especially infection!)