A 24 yo F with no PMH presents with 6 months of joint pain and puffy hands. Mother with systemic lupus erythematosus. ROS notable for Raynaud’s (view image) and mild dyspnea on exertion.
Physical Exam
- Synovitis of MCPs and wrists
- Pitting at distal fingertips (view image); nailfold capillaroscopy
- Normal pulmonary exam; RRR, prominent S2
Diagnostic Workup
- Labs:
- Hemoglobin 10.6, MCV 82; remaining CBC and BMP WNL
- High titer ANA, speckled pattern; high titer RNP; negative Smith, anti-SSA (RO antibody), anti-SSB, dsDNA, centromere, Scl 70, RF, CCP antibodies
- Imaging:
- CXR: normal lung fields
- TTE: dilated RV with normal function; normal LV size and function
Treatment & Further Workup
- Referral to rheumatology and cardiology!
- Hydroxychloroquine for MCTD and for inflammatory arthritis (weight-based dosing not to exceed 5 mg/kg)
- Calcium-channel blocker for Raynaud’s
- Right heart catheterization for workup of pulmonary artery hypertension
A 29 yo F presents with trouble going up and down stairs, trouble brushing her hair, and dyspnea on exertion.
Physical Exam
- Mildly puffy/swollen hands; no synovitis
- 4-/5 strength of BL iliopsoas and deltoids; otherwise normal neurologic exam
- Normal cardiopulmonary exam
- No rashes
- No tenderness over muscle groups
Diagnostic Workup
- Labs:
- High titer ANA, speckled pattern; high titer RNP; low complement; negative Smith, Ro, La, dsDNA, centromere, Scl 70, RF, CCP antibodies, myositis panel
- CK 1,037
- CBC shows platelets 120K
- Imaging:
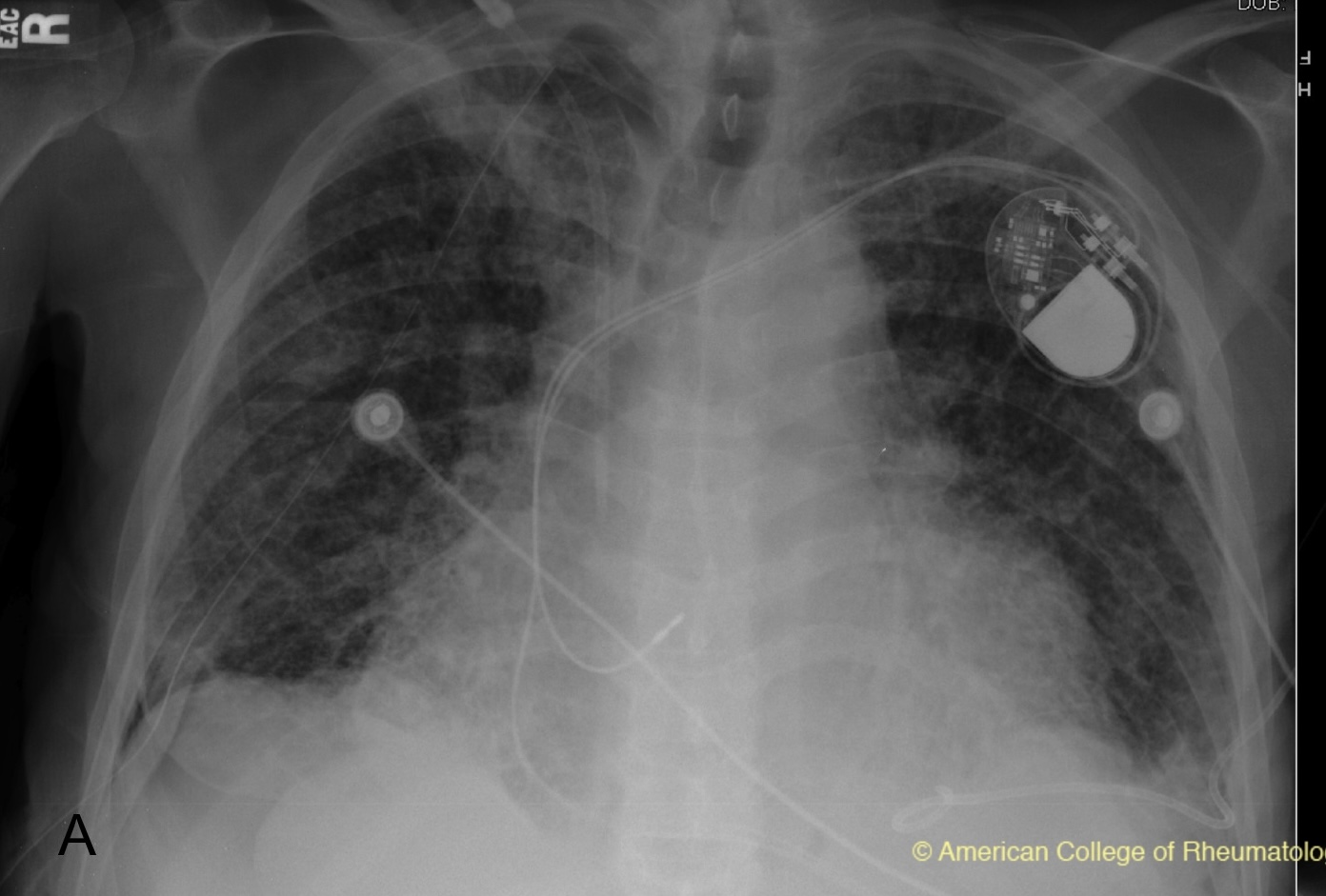
- CXR shows reticular opacities at the BL bases (view image); CT demonstrates NSIP pattern of interstitial lung disease (ILD) (view image); TTE normal
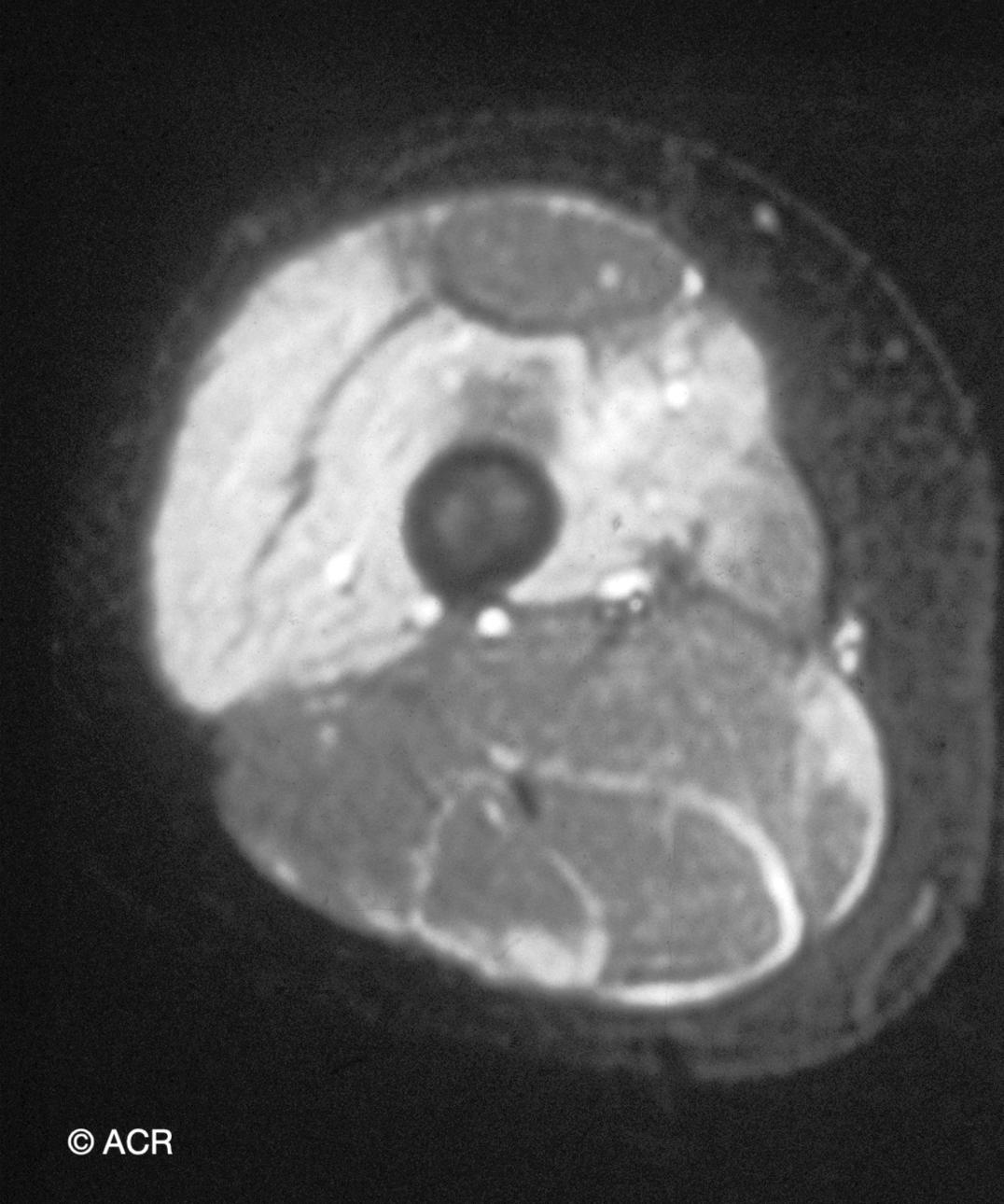
- MRI thigh with diffuse muscle edema (view image)
Treatment
- Prednisone 40 mg daily
- Neurology collaboration for trigeminal neuralgia and pulmonary collaboration for ILD
- Consider mycophenolate, azathioprine, or rituximab for ILD and myositis