About Mixed Connective Tissue Disease
Mixed connective tissue disease (MCTD) is a systemic, autoimmune connective tissue disease.
- Features of at least two of the following: lupus, rheumatoid arthritis, systemic sclerosis, and myositis; however, it is a distinct entity
- Female predominance
- Peak incidence: 20 yo
Most common features:
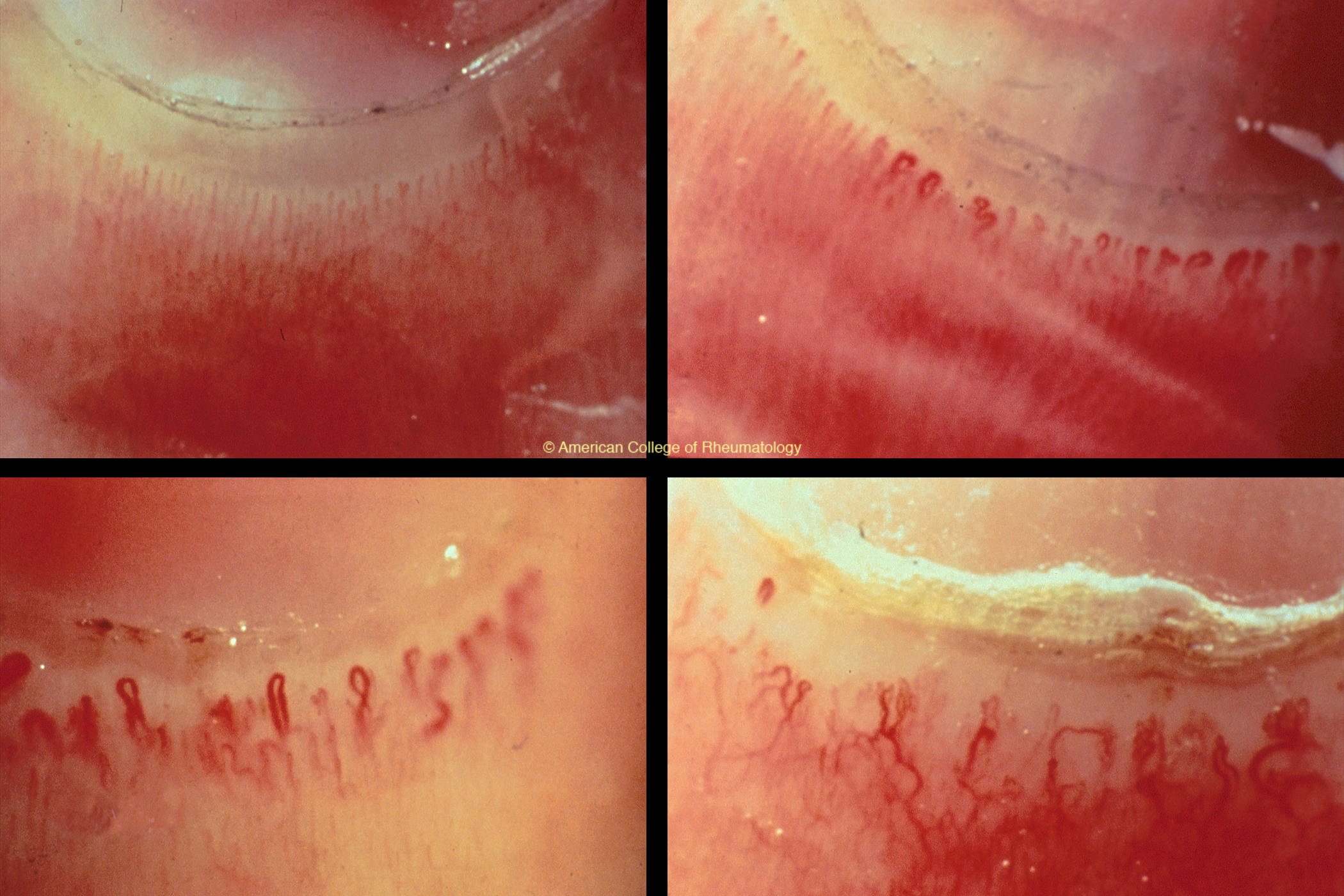
- Raynaud’s (~100%) (view image)
- Synovitis/arthritis
- Swollen hands, puffy fingers (view image)
- Myositis
Can also develop interstitial lung disease, PAH, rashes, and GI manifestations.
Typically develops gradually over time.
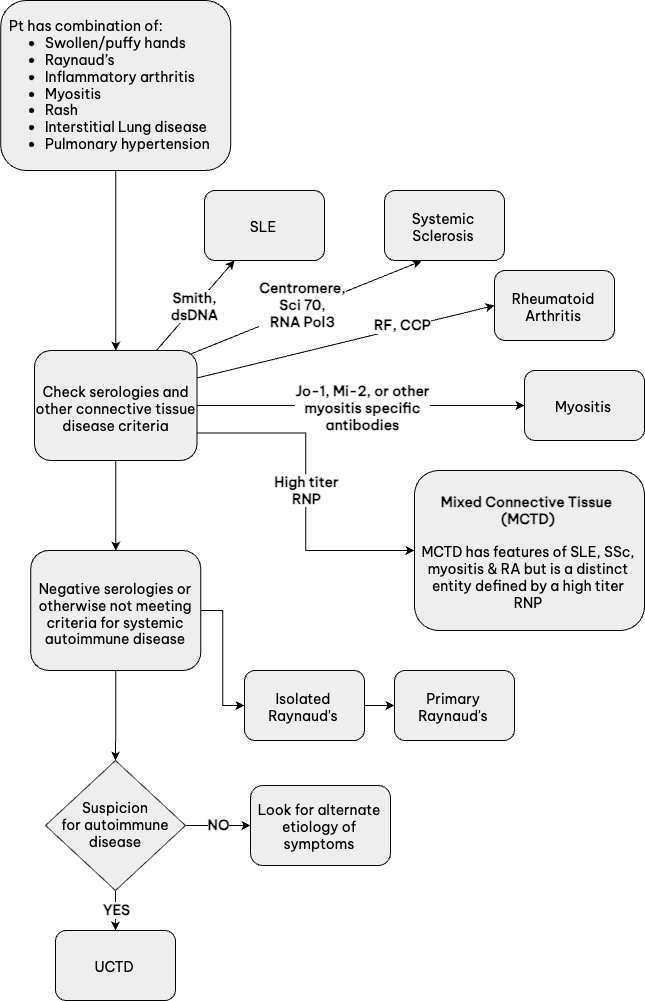
View recommended medical workup for MCTD
- Anti-ribonucleoprotein (RNP) antibody positivity is necessary for diagnosis.
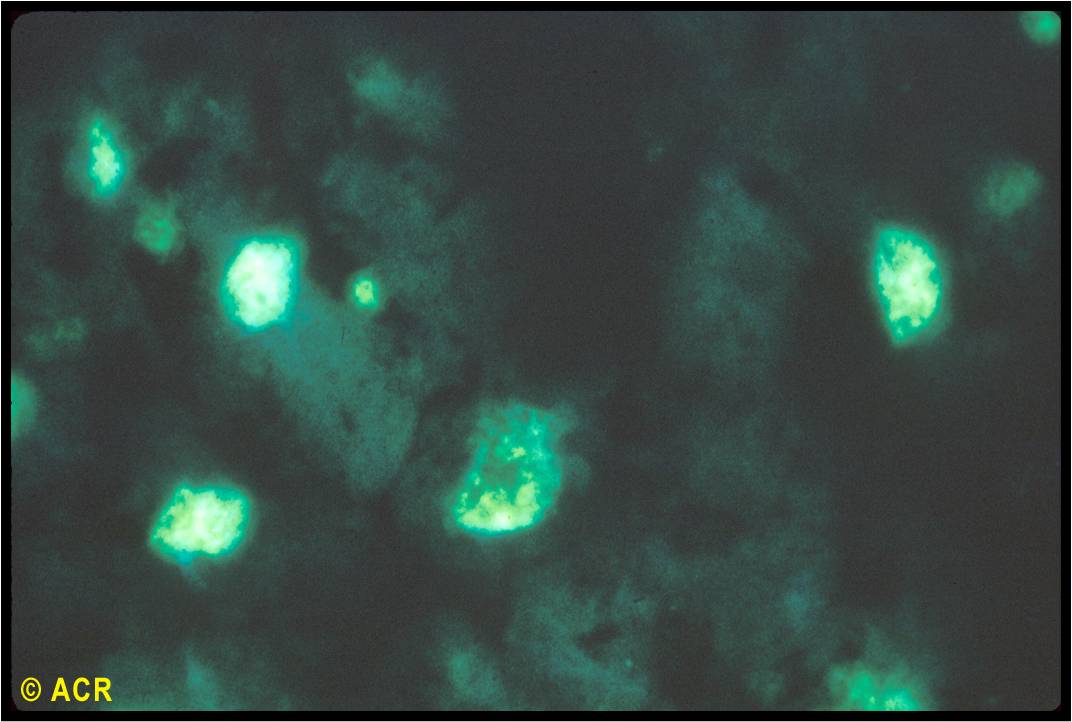
- Antinuclear antibody positive in all. (view image)
- If meets criteria of a different rheumatologic disease, consider overlap diagnosis.
- Systemic lupus erythematosus
- Systemic sclerosis
- Idiopathic inflammatory myopathy
- Rheumatoid arthritis
- Primary Raynaud’s
- Idiopathic pulmonary hypertension
- Undifferentiated connective tissue disease
Treatment depends on disease manifestations and requires collaborative care.
- Raynaud’s: Avoiding triggers, calcium channel blockers, topical nitroglycerin applied to the interdigital web spaces, PDE-5 inhibitors, SSRIs, and in severe cases, PDE-5 inhibitors or vasodilators like iloprost
- Arthritis: Disease-modifying anti-rheumatic drugs (DMARDs)
- Myositis: Immunomodulating medications like mycophenolate, methotrexate, IVIg, rituximab, etc.
- Sclerodactyly: Mycophenolate, etc., along with collaboration with dermatology
- Interstitial lung disease: azathioprine, mycophenolate, or rituximab
- For inflammatory manifestations, a prednisone taper is often required while waiting for other medications to take effect.
- Can evolve over time into another connective tissue disease. Raynaud’s tends to be severe and can progress to ulcerative lesions.
- Systemic sclerosis-like manifestations typically cause the most long-term morbidity and mortality.
- Pulmonary hypertension is a major cause of mortality.
- PFTs and echos can help screen for ILD and PAH.
- Systemic rheumatic disease with features of lupus, rheumatoid arthritis, systemic sclerosis, and/or myositis
- Raynaud’s phenomenon present in almost all patients (view image)
- Ribonucleoprotein (RNP) positivity is necessary for diagnosis:
- High-titer RNP=serological hallmark
- ANA negativity doesn’t rule out MCTD but makes MCTD incredibly unlikely diagnosis.
- Pulmonary HTN: major cause of mortality